Neuropsychiatry is a medical discipline that integrates the principles of neurology and psychiatry to manage mental health conditions with neurological origins. This specialty emphasizes the intricate relationship between brain function and behaviour, addressing disorders arising from brain injuries, dementia, or other neurological diseases. Neuropsychiatrists apply their dual expertise to diagnose and treat psychiatric symptoms linked to or resulting from nervous system dysfunctions.

Functional Neurological Disorder (FND) is a condition where the brain sends and receives signals incorrectly. It is often described using a "Computer Analogy."
"In FND, the hardware of the brain (the structures, nerves, and wires) is healthy and intact, but there is a problem with the software (the way the brain processes and sends information)."
Genuine Symptoms: The symptoms are real and often disabling. They are not "faked" or under the person's conscious control.
Inconsistency: Symptoms may fluctuate. For example, a tremor might disappear when the patient is distracted but return when they focus on it.
Reversibility: Because the problem is functional (software) rather than structural (permanent damage), there is significant potential for recovery.
FND is no longer a "diagnosis of exclusion" (only diagnosed when everything else is ruled out). Instead, specialists look for positive clinical signs that are unique to FND.
Limb weakness, paralysis, tremors, or "functional" tics.
Episodes resembling epilepsy but without abnormal electrical brain activity.
Numbness, tingling, or "vision tunnels" that don't follow nerve paths.
"Brain fog," sudden memory gaps, or difficulty word-finding.
A neurologist or neuropsychiatrist identifies FND through specific tests, such as:
Hoover’s Sign: Weakness in a leg that becomes strong when the patient is asked to move the other leg.
Entrainment: A tremor that changes its rhythm to match a movement the patient is making with their other hand.
Because FND sits at the intersection of mind and body, the most successful treatment involves a Multidisciplinary Team (MDT).
Physiotherapy: Retraining the brain to access "automatic" movement patterns (e.g., walking without thinking about it).
Neuropsychiatry/Psychology: Using Cognitive Behavioural Therapy (CBT) or Specialized Psychotherapy to address the "software glitch," manage stress, or treat co-occurring anxiety/depression.
Occupational Therapy: Helping patients adapt their daily routines and manage fatigue.
Speech and Language Therapy: Vital for those with functional speech or swallowing difficulties.
Neuropsychiatrists are uniquely trained to manage the "Why" and the "How" of FND. They treat the neurological symptoms while simultaneously addressing the psychological drivers—such as past trauma, high-stress environments, or maladaptive coping mechanisms—that may be fueling the brain's "software" errors.
Modern research has moved away from seeing FND as a purely "psychological" problem. As of 2025–2026, the scientific consensus describes FND as a disorder of brain network connectivity and predictive processing.
The brain is no longer viewed as a passive receiver of information, but as a "prediction machine" that has developed a glitch in its expectations.
Latest neuroimaging (fMRI) shows that in FND, specific brain networks are "talking" to each other too much or too little.
The Limbic-Motor "Hijack": Research shows increased connectivity between the Amygdala (the brain's emotional/threat centre) and the Supplementary Motor Area (SMA) (the part that prepares the body for movement).
• The Result: High emotional arousal or stress can "leak" directly into motor circuits, causing tremors or paralysis without the person's conscious intent.
The Salience Network Glitch: This network decides what is important to notice. In FND, the Insula and Anterior Cingulate Cortex (ACC) become hyper-aware of internal body sensations (interoception).
• The Result: The brain "over-amplifies" normal twitching or minor pain until it becomes a disabling symptom.
Right Temporoparietal Junction (RTPJ) Dysfunction: This area is responsible for the "Sense of Agency"—the feeling that "I am the one moving my arm."
• The Result: In FND, this area under-functions. Your arm might move (functional tic/tremor), but your brain fails to tag it as "self-generated," making it feel like someone else is moving your body.
This is currently the leading theoretical model for FND (supported by the latest 2025 Wartenberg Lecture and research by Prof. Jon Stone and others).
The "Prior" is Too Strong: Your brain constantly predicts what it will feel. If your brain "predicts" your leg is weak (perhaps due to a minor injury or high stress), it ignores the actual sensory data saying the leg is fine.
Top-Down vs. Bottom-Up: Normally, if you try to walk and your leg works, your brain updates its "map." In FND, the Top-Down prediction (the leg doesn't work) becomes so "loud" that it overrides the Bottom-Up evidence (the nerves and muscles are healthy).
The "Escalator Effect": Imagine stepping on an escalator that you think is moving, but it’s actually broken. You stumble because your brain's prediction didn't match reality. FND is like having that "stumble" sensation constantly.
Research in 2024–2025 has clarified why some people develop these faulty circuits while others don't. It is rarely one single cause, but a "perfect storm"
Childhood adversity or genetic "startle" sensitivity.
Sensitizes the Amygdala, making the brain more reactive to threat.
A physical injury, a bad migraine, or an acute panic attack.
Acts as the "trigger" that creates the first software glitch.
Anxiety about the symptoms, social isolation, or lack of diagnosis.
Reinforces the faulty Predictive Coding loop, making symptoms stick.
FND is the result of a brain that has become hyper-focused on its own internal predictions and has disconnected its emotional centres from its voluntary control centres.
The "hardware" is fine, but the integration of different brain regions is misaligned. This is why treatment involves "multimodal" therapy—you have to retrain the motor circuits while simultaneously calming the salience and limbic (emotional) circuits.
In the field of neuropsychiatry, "missed diagnosis" refers to two distinct risks: failing to identify FND in a patient (leading to unnecessary treatments) or incorrectly labelling a structural disease as FND (leading to delayed life-saving care).
Modern research indicates that the historical fear of a massive "misdiagnosis epidemic" is outdated, but the stakes for the individual remain high.
Misdiagnosis in this field typically occurs in one of two directions. Research shows that both directions occur at a similar rate - approximately 4% to 5%.
This occurs when a structural neurological condition is mistakenly diagnosed as FND.
Most common mimics: Multiple Sclerosis (MS), Parkinson’s Disease, and rare forms of Epilepsy.
The Risk Irreversible damage: If a patient has MS but is told they have FND, they miss the window for "Disease Modifying Therapies" (DMTs) that prevent permanent nerve scarring.
Why it happens: Over-reliance on "psychiatric triggers." If a patient with early-stage MS also has high anxiety, a doctor might "overshadow" the physical symptoms with the psychological ones.
This occurs when a patient’s functional symptoms are treated as structural damage.
Most common mimics: Treating functional seizures as "status epilepticus" or functional weakness as a stroke.
The Risk: Iatrogenic harm (harm caused by medical treatment). Patients may be unnecessarily intubated, given toxic anti-seizure medications, or undergo invasive surgeries.
Why it happens: Fear of missing a "catastrophic" illness. Doctors often prefer to over-treat a healthy person than under-treat a sick one, but in FND, this can reinforce the "faulty circuit" by convincing the brain it is more damaged than it is.
When an FND diagnosis takes years to confirm (the current average is often years), several secondary risks emerge:
Muscle Atrophy: Disuse of a "functional" limb can lead to actual muscle wasting or joint contractures.
Medical Gaslighting: Patients feel disbelieved, leading to "diagnostic trauma" and a breakdown in trust with the medical system.
Economic Drain: Studies show FND patients have higher healthcare costs before diagnosis due to repeated ER visits and unnecessary MRIs.
"Hard-Wired" Symptoms: The longer a faulty circuit is used, the harder it becomes to "retrain" via neuroplasticity.
Neuropsychiatrists now use the "Diagnosis of Inclusion" strategy to minimize these risks:
Don't rely on "Stress": Stress exists in everyone. Doctors should not diagnose FND just because you are stressed; they must find Positive Signs (like Hoover's sign).
Acknowledge Comorbidity: It is possible to have both. About 20% of people with FND have a co-existing neurological condition (e.g., someone with Epilepsy who also develops Functional Seizures).
Review the Hardware: If symptoms change or stop responding to therapy, the "hardware" (MRI/EEG) must be re-evaluated to ensure a new structural issue hasn't developed.
Research Fact: A systematic review by Stone et al. found that since 1970, the rate of misdiagnosis for FND has dropped significantly due to better imaging, yet the stigma of the diagnosis remains the biggest barrier to early treatment.
Functional Neurological Disorder (FND) can feel like being handed a complex manual written in a language you don’t quite speak yet. Because FND sits right at the intersection of neurology and psychiatry, your care plan needs to be equally "bilingual."
Here is a care-coordination checklist designed to help you navigate the first few months of treatment and ensure no part of your recovery is overlooked.
Phase 1: Confirmation and Education
The first step in "retraining the brain" is fully believing and understanding the diagnosis. Doubt acts like noise that interferes with the retraining process.
Request a "Positive Sign" Explanation: Ask your neurologist which specific clinical signs (like Hoover’s sign or entrainment) confirmed the diagnosis.
Education Resources: Visit reputable sites like FND Hope or Neurosymptoms.org. Understanding the "software vs. hardware" analogy is crucial.
Family Briefing: Share educational materials with family/friends so they understand your symptoms are real, but the brain's pathways are reversible.
Phase 2: Assembling Your Multidisciplinary Team (MDT)
FND is rarely treated by a single doctor. It takes a village—specifically, a neurological one.
Neuropsychiatrist: To oversee the "big picture" and manage any co-occurring mood or sleep issues.
Specialized Physiotherapist: Look for one with experience in FND (they focus on automatic movement rather than effortful strength).
Psychologist/OT: To help identify "triggers" (stress, fatigue, or sensory overload) and teach grounding techniques.
Phase 3: Immediate Management Strategies
While waiting for therapy appointments, these "first aid" steps can help manage daily symptoms.
The "Distraction" Toolkit: Identify activities that help reduce symptoms (e.g., listening to music, humming, or mental math).
Pacing Diary: Track your energy levels. Over-exertion often leads to a "crash" in functional symptoms.
Grounding Techniques: Learn "5-4-3-2-1" or weighted blanket techniques for when symptoms like functional seizures or dissociation occur.
Based on the world-leading FND resource Neurosymptoms.org (created by Professor Jon Stone), Functional Neurological Disorder symptoms are categorized into "Core FND Symptoms" and "Common Associated Symptoms."
These are the primary symptoms that define the disorder, often described as "software" glitches where the brain's signals are blocked or distorted.
Functional Limb Weakness: Weakness in an arm or leg that can feel like "paralysis" or heaviness.
Functional Tremor: Uncontrollable shaking that can vary in speed or disappear when distracted.
Functional Gait Disorder: Problems walking, such as dragging a leg, a "walking on ice" pattern, or sudden knee buckling.
Functional Dystonia: Spasms where a body part (like a hand or ankle) gets stuck in a fixed, often painful, position.
Functional Jerks and Twitches (Myoclonus): Sudden, shock-like jerky movements.
Functional Tics: Repetitive complex movements or vocal sounds.
Functional (Dissociative) Seizures: Episodes that look and feel like epileptic seizures or faints, but are not caused by abnormal electrical activity in the brain.
Functional Drop Attacks: Sudden falls to the ground without a "blackout" or loss of consciousness.
Functional Sensory Symptoms: Numbness, tingling, or "altered" sensations that don't follow typical nerve paths.
Functional Facial Symptoms: Spasms or weakness affecting the eye, eyelids, or lower face.
Functional Visual Symptoms: Blurred vision, double vision, or "visual field loss" (tunnel vision).
Functional Speech & Swallowing: Sudden stuttering, difficulty finding words, or a feeling of a "lump in the throat" (Globus).
Functional Cognitive Symptoms: Often called "Brain Fog"—problems with memory, concentration, or a feeling of "thinking through mud."
Functional Dizziness (PPPD): A persistent sense of swaying or unsteadiness.
Bladder Symptoms: Chronic urinary retention or overactive bladder issues without a structural cause.
Neurosymptoms.org emphasizes that while these are not "defined" as FND, they are incredibly common in FND patients and are often part of the same underlying "circuitry" issue.
Fatigue: Profound exhaustion that is not resolved by sleep.
Dissociative Symptoms: Feeling "spaced out," disconnected from your body (depersonalization), or that the world isn't real (derealization).
Chronic Pain: Including back/neck pain and fibromyalgia-type symptoms.
Sleep Problems: Insomnia or poor quality sleep.
Headaches: Including Migraines and tension-type headaches.
IBS & Gastric Issues: Irritable Bowel Syndrome or functional chest pain.
1. Hoover’s Sign (For Leg Weakness)
This is perhaps the most famous test for functional limb weakness.
The Test: The doctor asks you to push your "weak" leg down into the bed. It feels weak. Then, they ask you to lift your strong leg against resistance.
The Positive Sign: While you are focusing on the strong leg, the "weak" leg suddenly regains its strength and pushes down automatically.
What it proves: The "wires" to the leg are intact, but the brain is struggling to access that strength voluntarily.
2. The Entrainment Test (For Tremors)
This test looks at whether a tremor is "fixed" by brain structure or "fluid" based on brain attention.
The Test: If you have a tremor in your right hand, the doctor will ask you to copy a specific, different rhythm with your left hand.
The Positive Sign: The tremor in the right hand will either:
1. Change its rhythm to match the left hand (Entrainment).
2. Stop completely while you focus on the other hand.
3. Make it impossible for you to keep the rhythm in the "good" hand.
3. Tubular Vision (For Visual Symptoms)
In structural vision loss, the visual field expands the further away you get from an object.
The Positive Sign: In FND, the visual field may remain the same size regardless of distance (like looking through a cardboard tube). This is a classic sign of a functional processing change in the visual cortex rather than damage to the eye or optic nerve.
4. Hip Abductor Sign
Similar to Hoover’s sign, this test involves the patient pushing their legs outward.
The Positive Sign: Weakness in one hip disappears when the patient is asked to resist movement with the opposite hip.
5. Signature Signs of Functional Seizures
Unlike epileptic seizures, functional seizures often have specific "positive" markers:
Duration: They often last longer than 2–3 minutes.
Eyes: Eyes are frequently tightly closed (in epilepsy, they are usually open or flickering).
Side-to-side head movement: This is more common in functional episodes than in epilepsy.
Neuro-physiotherapy
Bypasses the "broken" conscious pathway to use automatic ones.
Cognitive Therapy
Addresses the "noise" (stress/anxiety) that jams the signals.
Occupational Therapy
Provides tools to navigate the world while the brain heals.
A Quick Reminder: Recovery in FND is rarely a straight line. It’s often "two steps forward, one step back," and that’s perfectly normal for a brain that's learning to reboot its software.
FND isn't just about recording what went wrong; it’s about finding patterns. Because FND is a "software" issue, your brain often reacts to hidden triggers like fatigue, sensory overload, or even "emotional echoes" from earlier in the day. This tracker is designed to help you and your neuropsychiatrist identify those glitches.
How to use this: Don't just list the symptom; list what was happening around it. Look for the "Pre-Symptom" state.
Cognitive Therapy
7
Walking in a loud mall
High stress, 5hrs sleep
Sat down, listened to music
At the end of each day, give yourself a quick score (1-5) on these three areas. Over time, you’ll likely see that when these scores are low, symptoms are high.
Physical Pacing: Did I stop before I was exhausted? [ 1 2 3 4 5 ]
Sensory Load: Was my environment calm or chaotic? [ 1 2 3 4 5 ]
Emotional Regulation: Did I acknowledge my feelings or push them down? [ 1 2 3 4 5 ]
FND recovery can feel slow. It is vital to track functional wins, no matter how small.
Example: "I felt a tremor starting but used a grounding technique to stop it before it escalated."
Example: "I walked to the mailbox without focusing on my legs."
Neuroplasticity Tip: When you record a "win," you are actually reinforcing the healthy neural pathways in your brain. You’re telling your "software" that it’s doing a good job.
When you go to your next appointment, don't just say "I'm having a hard time." Show them the tracker and say:
"I noticed my symptoms spike on Tuesdays after my loudest meeting, or whenever I get less than 6 hours of sleep. How can we adjust my 'Pacing Plan' to account for this?"
In the context of FND, grounding isn't just about "calming down"—it is a neurological tool used to redirect the brain's attention away from malfunctioning internal signals and back to the external environment. This helps "reset" the software glitch.
Here is a list of grounding techniques specifically categorized for FND management.
1. Sensory "Jolts" (To Break a Symptom Cycle)
These are high-intensity sensations designed to grab the brain's attention immediately. They are particularly useful for functional seizures or sudden paralysis.
The Ice Grip: Hold an ice cube in your hand for as long as you can. The cold signal is "loud" and can override internal FND signals.
Sour Power: Keep super-sour candies (like Warheads) or a slice of lemon nearby. The intense taste forces the brain to process a strong, real-time sensory input.
Strong Scents: Use smelling salts, peppermint oil, or eucalyptus. Olfactory (smell) signals have a very direct path to the brain’s emotional and regulatory centres.
2. Cognitive Distraction (The "Software Override")
FND symptoms often worsen when the brain "focuses" on them. These techniques force the brain to use its processing power elsewhere.
The Category Game: Pick a category (e.g., "Types of Cheese" or "80s Rock Bands") and name 10 items as fast as you can.
Reverse Math: Start at 100 and subtract 7 repeatedly ($100, 93, 86...$). This requires significant "working memory," leaving less room for the brain to maintain a functional symptom.
Object Description: Pick an object in the room and describe it in excruciating detail (texture, light reflection, shadow, weight, microscopic imperfections).
3. Physical "Automaticity"(For Motor Symptoms)
These techniques help the brain bypass "conscious" movement and return to "automatic" movement.
4. The "5-4-3-2-1" Method (TheGold Standard)
This is the classic grounding exercise, adapted for FND by focusing on externalizing your awareness
Grounding is a skill, like a muscle.
Practice when you are well: Don't wait for a major symptom flare to try these for the first time.
Identify your "Early Warning Signs": Use these techniques as soon as you feel "spacey," tingly, or "off."
Mix and Match: What works for a tremor might not work for brain fog. Find your personal "Top 3."
The secret is "Movement without Thinking." Since the "positive signs" proved that your muscles can work when the brain is distracted, these goals focus on tricking the brain into using those automatic pathways again.
Goal 1 : Utilizing the Hoover’s Sign Mechanism
The Logic: If your leg gets stronger when you focus on the other leg, we need to make movement a "secondary" task.
Target Activity: Standing or walking while performing a cognitive task.
Action Plan: * Practice standing up while naming 5 different colors in the room.
• Walk across the room while tossing a ball from hand to hand.
Success Marker: Moving the "weak" limb without consciously "willing" it to move.
Goal 2 : Breaking the Tremor Rhythm (Entrainment)
The Logic: We want to interfere with the brain’s "maladaptive" rhythm.
Action Plan: * If a hand tremor starts, immediately tap a complex, syncopated rhythm on the table with the opposite hand.
• Use a metronome set to a different speed than the tremor and try to match the metronome with your unaffected foot.
Success Marker: The tremor dampens or changes rhythm to match the new task.
Goal 3 : Restoring Gait (Walking) via "Glitches"
The Logic: Normal walking is automatic. FND walking often becomes "effortful" and heavy.
Target Activity: Bypassing the "manual" walk.
Action Plan: * Sideways/Backward Walking: The brain uses different circuits for these movements that are often unaffected by FND.
• Visual Cues: Place tape markers on the floor to "step over." This turns walking into a visual-spatial task rather than a motor-strength task.
Success Marker: Walking more fluidly when moving in a non-standard direction (sideways/backwards).
One of the biggest hurdles in FND rehab is overdoing it on a "good" day, which leads to a massive symptom flare-up the next day.
The 80% Rule: Always stop when you feel you have 20% of your energy left.
Quality over Quantity: Five minutes of "automatic" walking is better than twenty minutes of "struggling/dragging" walking.
Ensure your Physical Therapist (PT) and Neuropsychiatrist are aligned on these goals. Your PT focuses on the movement, while your Neuropsychiatrist helps manage the fatigue and anxiety that might be making the "software" glitch more frequently.
A brain injury—whether caused by a sudden trauma (Traumatic Brain Injury) or a medical event like a stroke or hypoxia (Acquired Brain Injury) — is never just a physical wound. It is a fundamental shift in how a person thinks, feels, and interacts with the world. Neuropsychiatry focuses on managing the "invisible" symptoms that often persist long after the physical scars have healed.

Brain injuries often affect specific "hubs" that regulate our personality and emotional control. The most commonly affected areas include the Frontal Lobes (the CEO of the brain) and the Temporal Lobes (the memory and emotion centre).
When these areas are damaged, the "brakes" of the brain are often removed, leading to:
Executive Dysfunction: Difficulty planning, organizing, or finishing tasks.
Emotional Lability: Rapid, often unpredictable shifts in mood (crying or laughing at inappropriate times).
Impulsivity: Acting without considering consequences, which can lead to social or financial strain.
The aftermath of a brain injury often involves a "constellation" of psychiatric symptoms that require specialized management.
Depression, Mania, Apathy
Occurs in up to 50% of patients in the first year post-injury.
PTSD, Generalized Anxiety, Panic
Often linked to the circumstances of the injury (e.g., a car accident).
Delusions, Hallucinations
Less common, but can occur with severe temporal lobe damage.
Irritability, "TBI Rage"
Often triggered by overstimulation or cognitive fatigue.
One of the most misunderstood aspects of brain injury is neuro-fatigue. Unlike normal tiredness, this is a profound exhaustion of the brain's processing power.
The Battery Analogy: A healthy brain starts the day with a 100% charge and uses 1% for a conversation. A brain-injured person may start at 50% and use 40% just to process the background noise of a busy grocery store.
Neuropsychiatric care for brain injury is not about "curing" the injury, but about maximizing function and quality of life.
Neuropharmacology: Using medications like stimulants (for processing speed), SSRIs (for mood), or mood stabilizers (for aggression) with a "start low, go slow" approach, as injured brains are more sensitive to side effects.
Cognitive Rehabilitation: Working with therapists to develop "compensatory strategies" (like using digital prompts or checklists) to bypass damaged circuits.
Environmental Modification: Reducing sensory overload (noise, bright lights) to prevent behavioural outbursts.
Family Education: Helping loved ones understand that "the person isn't being difficult; the brain is struggling."
Recovery from a brain injury is a marathon, not a sprint. A neuropsychiatric evaluation provides the roadmap for navigating the cognitive and emotional hurdles of that journey.
This checklist is designed to help families and caregivers bridge the gap between daily observations and clinical appointments. Tracking these changes helps your medical team fine-tune medications and therapy strategies.
Use this list to note the frequency and severity of symptoms over the past 2–4 weeks.
These symptoms are often the result of damage to the limbic system or frontal circuits.
Emotional Lability: Sudden, "out of blue" crying or laughing that doesn't match the person's actual mood.
Apathy: A profound lack of "get-up-and-go," often mistaken for laziness or depression.
Irritability: A "short fuse" where minor frustrations lead to significant outbursts.
Anxiety: Excessive worry about the injury itself or fear of social situations.
Documenting these helps the neuropsychiatrist understand the "cognitive load" the patient can handle.
Neuro-fatigue: Does the person "crash" mentally after a simple conversation or a 20-minute task?
Perseveration: Getting "stuck" on one idea, question, or activity and being unable to move on.
Processing Delay: A noticeable "lag time" between a question being asked and the person responding.
Executive Dysfunction: Difficulty starting a task, planning the steps, or finishing what they started.
Impulsivity: Spending money unwisely, making blunt/rude comments, or ignoring safety risks.
Social Cognition: Losing the ability to "read the room" or understand others' facial expressions/tones.
Disinhibition: Acting in ways that are uncharacteristic of their pre-injury personality.
These often act as "fuel" for psychiatric symptoms.
Sensory Overload: Becoming agitated in bright lights, crowded rooms, or noisy environments.
Sleep Disruption: Inability to fall asleep, or sleeping 12+ hours and still feeling exhausted.
Appetite Changes: Forgetting to eat or, conversely, being unable to stop eating (hyperphagia).
When you observe a specific behavioural incident (like an outburst), try to record it using this framework:
What happened right before?
"We were in a loud restaurant for 30 minutes."
What exactly did they do?
"Shouted at the waiter and began to cry."
What helped them calm down?
"Going to the quiet car and sitting in silence."
Pro Tip: If possible, keep a brief "Sleep and Mood" log for one week prior to the appointment. Often, a spike in behavioural issues correlates directly with a poor night's sleep.
Creating a "brain-friendly" environment is one of the most effective ways to reduce irritability and prevent neuro-fatigue. By lowering the amount of raw data the brain has to process, you preserve the patient’s limited mental energy for more important tasks, like rehabilitation and social connection.
Reducing Cognitive Load at Home
The brain uses a massive amount of energy to process visual information. Flickering lights or cluttered rooms can lead to "visual noise" that triggers headaches and irritability.
Swap the Bulbs: Replace cool-white or fluorescent bulbs with warm-colored LEDs. Use dimmers where possible.
Reduce Glare: Use "matte" screen protectors on tablets and TVs. Ensure sunlight isn't bouncing off mirrors or glass tables into the patient's direct line of sight.
Declutter Surfaces: A desk or kitchen counter covered in miscellaneous items forces the brain to constantly "filter" those items out. Keep only essential items visible.
For someone with a brain injury, background noise isn't just a distraction—it's physically painful and exhausting.
The "One-Sound" Rule: Ensure only one sound source is active at a time. If the TV is on, turn off the dishwasher or the radio.
Sound Dampening: Adding rugs, heavy curtains, or acoustic panels can stop sound from "bouncing" in rooms with hard floors, which reduces the auditory echo that causes fatigue.
Noise-Canceling Tech: High-quality noise-canceling headphones (even without music) can provide a "sensory reset" during high-stress times of the day.
Since the brain’s internal filing system is often damaged, we move that system to the physical environment.
Consistent Placement: Keys, wallets, and phones should have a designated "docking station." Never move them.
Transparent Storage: Use clear bins for clothes or kitchen items. Seeing the object removes the "mental search" step of trying to remember where things are hidden.
Visual Prompts: Place a dry-erase board in a central location (like the fridge) for the daily schedule. Use a "Don't Stop, Keep Going" sign on the bathroom door if the person often forgets the next step in their morning routine.
Fluorescent, bright, flickering.
Soft, indirect, warm-toned.
Open shelves with many colors/labels.
Items behind closed cabinet doors.
Hardwood or tile (loud, echoing).
Rugs or carpets (muffled sound).
Spontaneous, "play it by ear."
Predictable, written on a wall calendar.
Every home should have a designated "Quiet Zone" or "Low-Stimulation Pod." This is a corner or room where:
1. There are no screens or electronics.
2. Conversations are not allowed.
3. The lighting is very low.
4. Comfortable seating (like a beanbag or recliner) is available.
Encourage the patient to go here before they feel overwhelmed. Once a "meltdown" starts, it's often too late for the Quiet Zone to be fully effective.
Neuropsychiatry is a growing subspeciality under Medicine. Over the past century there has been a greater awareness in the dimensions of the Brain and Mind. Such exploration has bought new hopes to individuals struggling with complex disorders in the interactions between the brain and mind.
As the Brain and mind components are so closely wired together, any disruption to mutual circuits due to an injury or inflammation would result in disease of the mind. This would present with disturbance in mood, sleep, energy levels, motivation, memory and thinking. This is a Neuropsychiatry disorder and can be treated. If you have been diagnosed with a Neurological or Neurosurgical condition and your doctor or you believe you have comorbid mental health impact, you are best to consult a Neuropsychiatrist.
Traditionally these conditions would be managed by Psychiatrists, Neurologists and other neuroscience specialists. Such expectation has been lost in the vast array of expansion within their own fields.
Neuropsychiatrist uniquely get trained in this space allowing a better focussed approach to management and holistic treatment of such conditions. Today, we have new optimism to these conditions with greater scope of recovery especially when diagnosed and treated early.
A Neuropsychiatrist has a wide range of training. The bulk of the specialist’s time is spend within the Neuroscience space looking and studying brain images, examining key neurological signs and utilising specialised cognitive and bio marker tests to reach diagnostic conclusions. Yet, the primary strength of their work is in the understanding of complex psychiatric, neurological process and its interplay.
Neuropsychiatric consequences of Epilepsy
Neuropsychiatric consequences of Movement disorder e.g. Parkinson’s disease
Neuropsychiatric consequences of Brain Injury
Functional Neurological Disorders
Tics and Tourette’s disease
Cognitive/Memorydisorders
AutoimmunePsychosis
DissociativePhenomenon
The neuropsychiatry of movement disorders is a specialized field focusing on the complex intersection of motor control, emotion, and cognition. While movement disorders like Parkinson’s or Huntington’s are often defined by physical symptoms (tremors or stiffness), they are deeply intertwined with psychiatric conditions such as depression, anxiety, and behavioural changes.

At the heart of this field lies the basal ganglia, a group of subcortical nuclei responsible for "gatekeeping" both our movements and our moods. When these circuits are disrupted, the result is often a dual challenge: motor dysfunction and neuropsychiatric distress.
The primary neurotransmitter involved is dopamine. In neuropsychiatry, we often look at the "Goldilocks" principle of dopamine:
Too little dopamine: Leads to Parkinsonism (physical) and apathy/depression (psychiatric).
Too much dopamine: Leads to dyskinesia (physical) and psychosis/impulsivity (psychiatric).
Neuropsychiatric consequences of Parkinson's disease can include depression, anxiety, psychosis, apathy, and impulse control disorders. These symptoms can impact a person's quality of life and make it harder to treat the physical symptoms of Parkinson's.
Depression: A common symptom that can be endogenous or exogenous, apathetic or agitated
Anxiety: A common symptom that can include panic attacks
Apathy: A state of lethargy and loss of motivation
Psychosis: A symptom that can include hallucinations, illusions, and delusions
Impulse control disorders: A symptom that can include addictive patterns of drug use, gambling
Cognitive impairment: Can include dementia, which is a global impairment in cognition
Agitation or delirium: Can be related to antiparkinsonian drugs or other conditions like dehydration or infection
Historically, the psychiatric symptoms of these disorders were treated as "secondary" or "reactions" to the physical disability. Modern neuropsychiatry views them as primary biological symptoms caused by the same brain pathology affecting movement.
Clinical Insight: A patient with Parkinson’s may experience "off-period" anxiety, where their mood plummets exactly when their motor medication wears off. This proves that the motor and emotional circuits are physically linked.
Managing these conditions requires a multidisciplinary "whole-person" approach:
Pharmacotherapy: Careful balancing of dopaminergic drugs and psychotropics (SSRIs, antipsychotics).
Neuromodulation: Techniques like Deep Brain Stimulation (DBS) can improve movement but require careful psychiatric screening, as they can sometimes affect mood.
Psychotherapy: Cognitive Behavioral Therapy (CBT) adapted for neurological patients to manage the "identity shift" that comes with chronic illness.
Physical & Occupational Therapy: To maintain independence and boost self-esteem through movement.
This list is designed to help you and your care team look "under the hood" of Parkinson’s Disease. Often, neurologists focus on your gait and tremor because those are easy to see. These questions ensure the non-motor symptoms get the attention they deserve.
Take these questions to your next appointment. It can be helpful to have a family member or close friend answer them with you, as they may notice subtle shifts in your behaviour before you do.
1. Mood and Motivation
The "Apathy" Question: "I find myself sitting for hours not wanting to do anything, but I don't necessarily feel 'sad.' Is this depression, or is this Parkinson's-related apathy?"
The "Anxiety" Question: "Do my feelings of panic or worry get worse right before my next dose of Levodopa is due (the 'off' period)?"
The "Serotonin" Question: "Since Parkinson’s affects more than just dopamine, should we be looking at my serotonin or norepinephrine levels to help with my mood?"
2. Thinking and Memory (Cognition)
The "Processing" Question: "I feel like my brain is 'foggy' or that it takes me longer to find words. Is this normal aging, or is it part of the PD progression?"
The "Fluctuation" Question: "Are there specific times of day when my thinking is clearer than others? Does my medication affect my mental clarity?"
The "Multitasking" Question: "I’m struggling to follow recipes or manage my finances. Can we do a baseline cognitive screening today?"
3. Behaviour and Impulse Control
This is especially important if you are taking Dopamine Agonists (like Pramipexole or Ropinirole).
The "Compulsion" Question: "Have I started spending more money, eating more, or staying up late on the computer in a way that feels 'driven' or out of character?"
The "Personality" Question: "Has my partner noticed me becoming more irritable or 'shorter' with people lately?"
4. Sleep and Perception
The "Nightmare" Question: "Am I acting out my dreams—kicking, punching, or shouting in my sleep? (This is known as REM Sleep Behaviour Disorder)."
The "Shadow" Question: "Am I seeing 'flickers' or 'shadows' out of the corner of my eye that aren't there? Are these early hallucinations caused by my medication?"
Track your mood specifically during times when your motor symptoms are at their worst.
A spouse or child can report behavioural changes like irritability that the patient might not perceive.
Pick the top two non-motor symptoms that bother you most. Don't try to solve all of them in one visit.
A Note on Candor: Don't be embarrassed to mention things like hypersexuality or gambling urges. These are medical side effects, not moral failings. Your doctor needs to know so they can adjust your "dopamine budget."
Managing Parkinson’s disease (PD) alongside mental health conditions like depression or anxiety is a delicate balancing act. Because PD medications increase dopamine and many psychiatric drugs affect serotonin or block dopamine, they can sometimes "clash."
This guide summarizes the key interactions you should discuss with your neuropsychiatrist or neurologist.
These combinations require careful monitoring by a specialist.
(e.g., Selegiline, Rasagiline)
SSRIs/SNRIs (e.g., Prozac, Zoloft, Effexor)
Serotonin Syndrome: A rare but serious condition of "serotonin overload" causing confusion, high fever, and muscle rigidity.
(Sinemet)
Typical Antipsychotics (e.g., Haloperidol, Risperidone)
Dopamine Blockade: These psychiatric meds "cancel out" your PD meds, potentially causing a severe worsening of tremors and stiffness.
(Apokyn)
Ondansetron (Zofran)
Severe Hypotension: Can lead to a dangerous drop in blood pressure or loss of consciousness.
These medications are generally preferred because they have a lower risk of interfering with your motor control.
For Psychosis: Quetiapine (Seroquel) or Clozapine are often used at very low doses. Pimavanserin (Nuplazid) shows promises as it targets serotonin without blocking dopamine receptors.
For Depression: Sertraline (Zoloft) and Citalopram (Celexa) are often well-tolerated, provided they are started at low doses and monitored if you are also on an MAO-B inhibitor.
For Anxiety: Cognitive Behavioural Therapy (CBT) is often the preferred "medication-free" start, but SNRIs like Venlafaxine can be effective for both pain and anxiety in PD.
When we treat Parkinson's, we are trying to fill a "dopamine tank" that has a leak.
If the tank is too empty: You experience tremors, stiffness, and depression.
If the tank is too full (over-replacement): You may experience dyskinesia (wiggly movements) or Impulse Control Disorders (ICDs).
Important Note on Impulse Control: If you are taking a Dopamine Agonist (like Pramipexole or Ropinirole), adding certain antidepressants can occasionally change how your brain processes "rewards." If you notice a sudden urge to gamble, shop excessively, or eat uncontrollably, tell your doctor immediately. This is a chemical side effect, not a lack of willpower.
While rare, it is vital to know the difference between a reaction to too much serotonin and a reaction to stopping dopamine.
Too much serotonin (often MAO-B + SSRI).
Fast heart rate, shivering, sweating, hyper-reflexes (twitchy).
Sudden stop of PD meds or starting heavy dopamine blockers.
Extreme muscle "lead-pipe" rigidity, very high fever, mental confusion.
Managing these medications is a team effort. Never stop a psychiatric or PD medication "cold turkey," as this can trigger a medical emergency.
Caring for the Mind While Supporting the Body
When a loved one has Parkinson’s, you aren't just managing appointments and medications—you are often navigating a profound shift in their personality and your relationship. This guide is designed to help you stay grounded when the "invisible" symptoms become overwhelming.
It is normal to feel a sense of grief, even though your loved one is still here. Neuropsychiatric symptoms like apathy or personality changes can make you feel like the person you knew has slipped away.
Validation: Remind yourself daily: “The disease is talking, not my spouse/parent.”
Separate the Person from the Pathology: When they are irritable or impulsive, it is often a "misfire" in their frontal lobe or a dip in their dopamine, not a personal attack on you.
When cognitive "fog" or irritability sets in, standard communication often fails. Try the Three-S approach:
Short: Use one-step instructions. Instead of "Let's get your coat, find your shoes, and head to the car," try "Let's put on your coat."
Simple: Avoid "why" questions (e.g., "Why are you acting like this?"). These require complex abstract thinking that the brain may no longer be able to provide.
Slow: Give the brain 10 to 20 seconds to process a question before repeating it. Silence is your best tool.
Loss of dopamine in the "reward" centre.
Don't ask, just do. Instead of "Do you want to walk?", say "It's time for our 5-minute walk," and hand them their shoes.
Chemical imbalance or med side effects.
Validate the emotion, not the vision. "I don't see the person in the corner, but I can see that it's making you feel scared. Let's go into the kitchen."
"Thin" emotional brakes.
The 10-foot Rule. If they are escalating, physically move 10 feet away. Reducing your physical "presence" can lower their sensory input and de-escalate the situation.
You cannot pour from an empty cup. Caregiver burnout isn't just "tiredness"; it's a physiological state that mirrors the patient's own stress.
Schedule "Identity Time": Spend at least 30 minutes a day doing something that has nothing to do with being a caregiver (reading, a hobby, calling a friend).
Build a "Respite Bridge": Don't wait for a crisis to find a backup. Research local respite care or "adult day programs" now, so the transition is easier later.
The "Good Enough" Rule: Some days, "good enough" care is a victory. Let go of the guilt of not being a perfect therapist, nurse, and spouse all at once.
A Final Thought: You are the most important part of your loved one's treatment plan. By protecting your own mental health, you are providing them with the stable, calm environment their brain needs to function at its best.
Understanding the "Triad" of Symptoms
Huntington’s Disease (HD) is a unique and challenging genetic condition. Unlike many other neurological disorders, HD is defined by a "Triad" of symptoms: Motor, Cognitive, and Psychiatric. While the "chorea" (involuntary dancing movements) is the most visible sign, the neuropsychiatric symptoms often appear years earlier and can be the most distressing for both the individual and their family.
The Biological Root: The Striatum
HD is caused by a genetic mutation that leads to the progressive breakdown of nerve cells in the brain, particularly in the striatum (part of the basal ganglia). The striatum acts as the brain's "volume knob" for both movement and emotion.
When the striatum atrophies, the "brakes" on behaviour and movement are released. This leads to the characteristic physical movements and the "disinhibited" or impulsive behaviours seen in neuropsychiatry.
The Huntington’s Triad
Chorea (twisting), rigidity, slurred speech.
Can lead to social withdrawal and "movement anxiety."
Difficulty planning, "getting stuck" on ideas.
Known as "executive dysfunction"; causes frustration.
Irritability, apathy, depression, OCD.
Often the most disabling part of the disease for families.
This is often the most difficult symptom for caregivers. It isn't "anger" in the traditional sense; it is a biological inability to regulate frustration.
The Cause: The frontal lobes lose their ability to "filter" impulses.
The Trigger: Sudden changes in routine or complex questions can cause a "meltdown."
Apathy is the most common psychiatric symptom in HD. The person may sit for hours and show no interest in hobbies they once loved.
Clinical Note: This is often misdiagnosed as depression, but unlike depression, the person may not feel "sad"—they simply lack the "spark" to start an activity.
A person with HD may ask the same question repeatedly or become obsessed with a specific idea (e.g., wanting to go to the store now). This is a result of the brain's "switching" mechanism being damaged.
Because HD is a "family disease," the treatment must be multidisciplinary.
Medication Balancing: Using medications like Tetrabenazine for movement and SSRIs or Antipsychotics for irritability and mood.
Routine is Medicine: A highly predictable daily schedule reduces the "cognitive load" and prevents irritability.
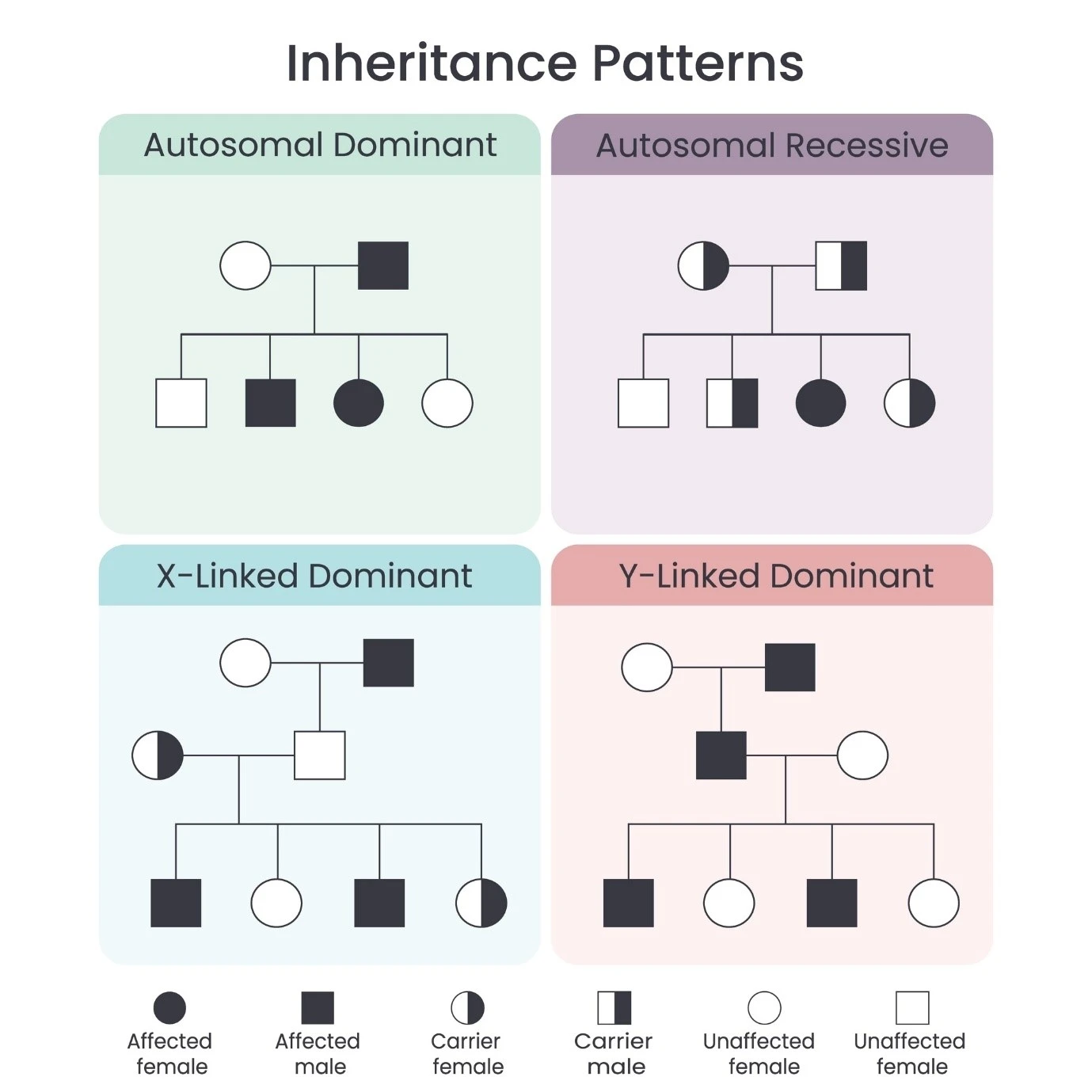
Genetic Counseling: Since HD is autosomal dominant, neuropsychiatric care often includes supporting the mental health of children and relatives who may be at risk.
The Neuropsychiatrist's Role: In HD, the goal is to "smooth out" the emotional peaks and valleys. By stabilizing the psychiatric symptoms, we allow the person to remain engaged with their family for as long as possible.
This requires a shift from "persuading" to "facilitating." Because the brain’s "switching" and "filtering" mechanisms are physically damaged, traditional arguments or logic often fail.
This toolkit provides actionable strategies to handle the two most challenging behavioural symptoms: Perseveration and Irritability.
Perseveration happens when the brain gets stuck on a loop—a single question, a specific task, or a perceived need. It is not "stubbornness"; it is a failure of the brain's internal gear-shifter.
The "Later" Card: If a loved one is stuck on a request (e.g., "I want a soda" repeated 20 times), write the answer on a card: "We will have soda at 4:00 PM." Point to the card instead of repeating yourself. This offloads the memory task from their brain to the environment.
Forced Choice: Instead of an open-ended "What do you want to do?", offer two specific options: "Do you want to walk to the park or sit on the porch?"
The Pivot: Don't argue with the "stuck" thought. Acknowledge it once, then physically change the environment (e.g., move to a different room or turn on music) to help the brain reset.
Irritability in HD is often a "thunderstorm" in the brain caused by sensory overload or a sudden change in plans. The "brakes" that normally stop an angry impulse are simply no longer there.
Reduce the "Data Stream": If you see signs of irritability (pacing, louder voice), turn off the TV, dim the lights, and stop talking. Lowering the sensory "volume" can prevent a full outburst.
Avoid the "Why": Never ask "Why are you acting like this?" It requires abstract reasoning that is often lost in HD. Instead, use "I" statements: "I can see you're frustrated. Let's take a break."
The 10-Foot Rule: If an outburst occurs, give the person physical space. Moving 10 feet away reduces the perceived "threat" to their overstimulated brain and allows the adrenaline to dissipate.
Use this table as a quick reference for daily interactions.
"Stop asking me that!"
"I wrote the answer on the fridge."
Uses visual cues to bypass damaged memory circuits.
"Hurry up and choose."
"Take your time. I'll check back in a minute."
Respects the processing delay (bradyphrenia) common in HD.
"We're going to the store, then the bank, then lunch."
"We are going to the store now."
Prevents cognitive "bottlenecking" and overwhelm.
Detailed explanations.
Short, 5-word sentences.
Keeps the "mental load" low and manageable.
Predictability is the best "medication" for HD irritability. When the brain knows what is coming next, it doesn't have to work as hard to process the world.
The Master Calendar: Use a large, visible wall calendar for all appointments.
Object Prompts: If it’s time for a walk, place the person's shoes in their line of sight rather than telling them to "get ready."
Consistent communication can significantly lower the need for sedative medications.
This plan is a vital document for any household or care setting dealing with Huntington’s Disease (HD). Because "HD Rage" is a biological event—akin to a seizure of the emotional centers—traditional "parenting" or "policing" techniques will fail. This protocol focuses on safety, de-escalation, and dignity.
A Guide for Family, Friends, and Visiting Staff
Before a full outburst, there is usually a buildup of internal pressure.
Signs: Increased pacing, louder or faster speech, repetitive questioning (perseveration), or flushed skin.
The Goal: Reduce the sensory "load" before the "brakes" fail completely.
Action: * Stop the conversation. Immediately stop explaining or arguing.
Lower the volume. Turn off the TV, radio, or loud appliances.
Provide an "Exit": Say, "I’m going to go to the kitchen to get some water; I'll be back in five minutes." This gives them space without making them feel "sent to their room."
At this stage, the frontal lobe (the logic center) has essentially "gone offline." The person is in a fight-or-flight state.
The Safety Protocol:
Maintain Distance: Stay at least 6–10 feet away. Do not try to touch them or "hug it out," as this can be perceived as an attack.
Use "Low and Slow" Speech: Speak in a calm, monotone voice. Use very few words.
No Eye Contact: Intense eye contact can be seen as a challenge or a threat to a brain in crisis. Look slightly to the side.
Remove Targets: If there are children or pets in the room, quietly usher them out first.
Identify the Exit: Always ensure you are between the person and the door. Never let yourself be cornered.
After the adrenaline drops, the person with HD will often feel profound exhaustion, confusion, or even shame.
Do NOT Lecture: Do not ask "Why did you do that?" or demand an apology. Their brain likely cannot process the sequence of events yet.
Encourage Rest: The brain needs to "reboot." Encourage a nap or a quiet period in a dark room.
Hydrate: Physical outbursts are exhausting; offer a cool drink.
Share this table with any new healthcare worker or guest.
Give 6ft of personal space.
Prevents sensory "crowding."
Keep hands visible and still.
Unexpected touch can trigger a "startle" rage.
Agree or distract.
Logic is not accessible during an HD event.
Look at the floor or a neutral object.
Reduces the "threat" response in the amygdala.
If the person becomes a danger to themselves or others, or if a weapon is involved, it is a medical emergency. Contact emergency services or the local AE mental health team.
Epilepsy is more than a tendency to have recurrent seizures; it is a complex neurological condition that frequently involves psychiatric symptoms. The field of neuropsychiatry focuses on understanding how these seizures, the underlying brain dysfunction, and the treatments used affect a person's mood, cognition, and behaviour.

Neuropsychiatric consequences of epilepsy can include a range of mental health issues often arising from the direct impact of seizures on the brain, the social stigma associated with epilepsy, and potential side effects of anti-seizure medications; with a complex bidirectional relationship where epilepsy can trigger psychiatric symptoms and pre-existing mental health conditions can exacerbate seizure activity.
Psychiatric disorders are significantly more common in people with epilepsy (PWE) than in the general population. This is often due to shared biological pathways rather than just a reaction to having a chronic illness.
~30% - 50%
Often presents as "interictal dysphoric disorder" (irritability, insomnia, and mood swings).
Anxiety ~20% - 25%
Can include generalized anxiety, panic attacks, or fear related to seizure occurrence.
~2% - 7%
May occur after a cluster of seizures (postictal) or independently (interictal).
High in Children
Often linked to frontal lobe dysfunction or the side effects of medications.
In neuropsychiatry, we categorize symptoms based on when they occur in relation to a seizure. This helps doctors determine the best treatment path.
Pre-ictal: Symptoms like irritability or "prodromal" mood changes hours before a seizure.
Ictal: Psychiatric symptoms occurring during the seizure (e.g., sudden intense fear, déjà vu, or hallucinations).
Post-ictal: Confusion, depression, or psychosis occurring immediately after a seizure, sometimes lasting for days.
Interictal: Psychiatric symptoms that occur between seizures, often representing a chronic state.
The relationship between epilepsy and psychiatry is bidirectional. This means that people with depression are more likely to develop epilepsy, and vice versa.
The Limbic System (including the hippocampus and amygdala) plays a dual role: it is the most common site for focal seizures (Temporal Lobe Epilepsy) and the primary center for emotional regulation. When these circuits are disrupted by electrical "storms," both movement and mood are affected.
Key biological factors include:
Neurotransmitter Imbalance: Changes in GABA (inhibitory) and Glutamate (excitatory) levels.
HPA Axis Dysregulation: Chronic stress responses affecting brain chemistry.
Structural Changes: Sclerosis or scarring in the temporal lobes.
Managing neuropsychiatric symptoms in epilepsy requires a delicate balance. A multidisciplinary approach is essential.
Some Antiseizure Medications (ASMs) can impact mood:
Mood Stabilizers: Medications like Valproate or Lamotrigine can help both epilepsy and bipolar symptoms.
Negative Impact: Medications like Levetiracetam (Keppra) may occasionally cause irritability or "Keppra-rage" in sensitive individuals.
Because of the stigma often associated with both epilepsy and mental health, therapy (CBT) and support groups are vital for improving the quality of life.
Important Note: Stopping or changing seizure medications without medical supervision can lead to status epilepticus (prolonged seizures) or a rebound in psychiatric symptoms. Always consult your neurologist and neuropsychiatrist before making changes.
Mood disorders:
Depression and anxiety are the most common neuropsychiatric complications, often linked to the stress of living with epilepsy, fear of seizures, and social isolation.
Psychosis:
Some individuals with epilepsy can experience psychotic episodes, including hallucinations and delusions, either during or after seizures (postictal psychosis) or even between seizures (interictal psychosis).
Cognitive impairment:
Epilepsy can lead to difficulties with memory, attention, executive functioning, and processing speed, which can impact daily life and learning abilities.
Behavioral changes:
Some individuals with epilepsy might exhibit behavioural changes like irritability, aggression, or social withdrawal.
Autism spectrum disorder (ASD):
Studies suggest a potential link between epilepsy and ASD, especially in children.
Impact of antiepileptic medications:
Certain anti-seizure medications can have side effects that contribute to neuropsychiatric symptoms like fatigue, mood swings, and cognitive impairment.
Factors contributing to neuropsychiatric consequences:
Severity of epilepsy:
Individuals with frequent or severe seizures are more likely to experience neuropsychiatric symptoms.
Brain region affected:
The specific brain area (brain circuits) where seizures originate can influence the type of neuropsychiatric symptoms experienced.
Social stigma:
The stigma associated with epilepsy can lead to isolation, low self-esteem, and increased anxiety.
Diagnosis and management:
Comprehensive evaluation:
A thorough assessment by a healthcare professional usually your GP, Neurologist, including a neurological examination, EEG, and psychological evaluation, is crucial to identify neuropsychiatric symptoms. Prompt your specialist to think ‘Neuropsychiatry’ as depending on specialisation and expertise such symptoms can be missed.
Treatment options:
Depending on the symptoms, treatment may include:
Optimizing seizure control: Effective seizure management with antiepileptic medication is often the first step.
Psychotherapy: Cognitive behavioral therapy (CBT) can be beneficial for managing anxiety, depression, and coping skills.
Psychiatric medication: In some cases, additional psychiatric medication may be needed to address specific symptoms.
Selecting an antiseizure medication (ASM) often involves a "buy one, get one" approach: a drug might help control your seizures while also treating a mood disorder, or it might unfortunately worsen it.
Here is a detailed breakdown of how common medications can influence your neuropsychiatric health.
The effects of these medications can generally be categorized into positive (psychotropic/stabilizing), negative (depressant/irritating), or mixed.
Lamictal
Often acts as an antidepressant. Highly effective for bipolar depression and overall mood stability.
Depakote
A powerful mood stabilizer. Excellent for controlling mania, aggression, and impulsivity.
Keppra
Can cause "Keppra-rage" (extreme irritability, hostility, or agitation) and depression in sensitive users.
Topamax
Known for "cognitive fog": word-finding difficulties, slowed thinking, and increased risk of depression.
Neurontin
Often has anxiolytic (anti-anxiety) effects and can improve sleep quality. But can cause the brain fog.
Fycompa
Carries a "Black Box" warning for serious behavioral changes, including aggression and suicidal ideation.
Tegretol
Used to treat mania and can help stabilize mood, similar to valproate.
Luminal
High risk of depression, lethargy, and hyperactivity (paradoxical) in children.
These are two of the most common patient-reported side effects in the epilepsy community:
Keppra-Rage: A sudden, intense irritability or anger that feels "out of character." It often responds well to Vitamin B6 supplementation, though you must consult your doctor first.
Topamax-Fog: Cognitive slowing where patients feel like they are "thinking through molasses" or struggle to find common words during a conversation.
In rare cases, a patient’s seizures are finally brought under control (the "normalization" of the EEG), but as the seizures disappear, psychiatric symptoms like psychosis or severe anxiety suddenly emerge. It is as if the brain used the seizure activity to "vent" electrical energy, and stopping them creates a different kind of pressure.
Most psychiatric side effects are dose-dependent. Starting at a very low dose and increasing it slowly (titration) allows the brain to adapt, significantly reducing the risk of a negative mood reaction.
Pro-Tip: If you have a personal or family history of depression or anxiety, mention this to your neurologist. They may choose a "mood-positive" medication like Lamotrigine to support your mental health while treating the epilepsy.
Tracking the relationship between your seizures and your mood is one of the most powerful things you can do for your care team. Since memory can be a bit "foggy" (especially after a seizure or on certain meds), having a paper or digital trail turns "I think I’ve been moody" into "I’ve had 4 days of high irritability following my last seizure."
Here is a structured template you can print or copy into a notes app.
Focal (2 min)
3/10
High irritability (Rage)
Missed morning dose; poor sleep.
When filling out the "Primary Mood Symptom" column, look for these common neuropsychiatric markers:
Keppra-Rage: Snap-irritability or "short fuse."
Topamax-Fog: Slowed thinking, word-finding trouble, or "zombie" feeling.
Interictal Dysphoria: Chronic, low-grade sadness or irritability between seizures.
Post-ictal Depression: A sudden "crash" in mood immediately after a seizure occurs.
Anxiety/Aura: Feeling a sense of impending doom or "fear" that precedes a seizure.
Look for Patterns: Does your mood dip 24 hours before a seizure? That might be a "prodrome" signal. Does it crash after? That’s post-ictal.
Highlight the "Medication Start" Date: If you started a new ASM on the 10th and your mood score dropped on the 12th, that is vital data for your doctor.
Be Brutally Honest: Doctors are used to hearing about "the rage" or "the fog." They can't adjust your meds to help your quality of life if they don't know the full story.
A Note on Safety: If you track a mood score of 1 or 2, or experience thoughts of self-harm, do not wait for your next appointment. Contact your neurologist or neuropsychiatrist immediately.
When you head into your next appointment with your data in hand, you want to move the conversation from "I feel bad" to "How do we fix this clinically?"
Here is a list of targeted questions categorized by the specific issues you might be seeing in your tracker.
If your mood shifts seem to "orbit" your seizures:
Post-Ictal Management: "I feel severely depressed for 48 hours after a seizure. Is this a 'post-ictal' symptom of the seizure itself, and is there a way to manage that recovery window better?"
The Aura/Anxiety Link: "I feel intense fear right before a seizure starts. Is this fear an 'aura' (part of the seizure), or is it an anxiety attack triggered by the anticipation of the seizure?"
Forced Normalization: "Since my seizures have stopped, my anxiety has actually gotten worse. Could this be 'forced normalization,' and how do we balance my brain chemistry now?"
If your main struggle is thinking clearly
Drug vs. Disease: "Is my cognitive slowing caused by the seizures themselves causing 'wear and tear,' or is it a side effect of the high dosage of my current medication?"
Neuropsychological Testing: "Would it be beneficial for me to have a formal neuropsychological evaluation to map out my cognitive strengths and weaknesses?"
The Specialist Referral: "Do you work with a Neuropsychiatrist? I think I would benefit from a doctor who understands exactly how my epilepsy and my mental health interact."
Emergency Protocol: "If my mood tracker shows a sudden drop into suicidal ideation or extreme aggression, what is the 'after-hours' protocol for adjusting my seizure meds safely?"
Doctors are often short on time. Start with: "I've been using a mood tracker, and I've found a consistent pattern of [X] happening [Y] days after my seizures. I'd like to review my medication's role in this."
The field of neuropsychiatry in epilepsy has shifted rapidly in the last 24 months (2024–2026). The focus has moved from merely "managing side effects" to precision neuropsychiatry, where we use specific medications to treat both the seizures and the underlying brain network dysfunction simultaneously.
Here is a summary of the most recent evidence and clinical shifts as of 2026:
The most significant breakthrough in 2025–2026 is the clinical trial data for XEN1101 (a potassium channel opener).
The Evidence: Unlike traditional ASMs that may worsen mood, XEN1101 is being studied specifically for its fast-acting antidepressant effects alongside its seizure-control capabilities (Phase 2 X-NOVA trials).
The Clinical Shift: We are entering an era where a single drug might be prescribed specifically because a patient has both epilepsy and treatment-resistant depression.
Recent real-world data (late 2025) has provided a surprising update on Cenobamate, one of the most powerful new drugs for focal seizures.
The Evidence: While high doses can cause somnolence, 2025 studies showed that many patients experienced a significant improvement in memory and executive function after 18 months.
The Mechanism: This wasn't necessarily a direct "pro-cognitive" effect of the drug, but rather a "secondary benefit" caused by the drug's high efficacy, which allowed doctors to simplify polytherapy and remove older, more "foggy" medications.
Validated in 2025, the Seizure Related Impact Assessment Scale (SERIAS) has become the "gold standard" for neuropsychiatric tracking.
The Evidence: Research showed that patients’ self-reported "time lost" (to either seizures or side effects) was a better predictor of long-term mental health than the actual number of seizures.
The Implementation: Clinics are now moving toward "patient-centered outcomes" where a drug is considered a failure if the "mood cost" exceeds the "seizure benefit," even if the patient is seizure-free.
There is mounting evidence (2025-2026) linking chronic neuro-inflammation to the "psychosis of epilepsy" and "forced normalization."
The Evidence: Elevated levels of the inflammatory marker Interleukin-1β (IL-1β) have been found in both the hippocampus of epilepsy patients and the blood of those with treatment-resistant depression.
The Future: Anti-inflammatory therapies (like IL-1R antagonists) are currently being explored as "neuroprotective" additions to seizure regimens to prevent long-term cognitive decline.
The International League Against Epilepsy (ILAE) updated the seizure classification system in 2025.
The Change: The system now places a heavier emphasis on "Consciousness" (replacing "Awareness") and observable vs. non-observable manifestations.
Neuropsychiatric Importance: This helps clinicians better identify "non-motor" seizures that look like psychiatric events (like panic attacks or "blank stares"), reducing the average 5–10 year delay in correctly diagnosing neuropsychiatric epilepsy.

At “All Psychiatry” our team of Australian- certified mental health clinicians provides expert care tailored to your needs.
We have made it simple and efficient - just follow the steps below to get started

To get started, please obtain a referral from your GP addressed to “All Psychiatry” and include as much information as possible.
It helps to include information about your symptoms, history and any previous treatment.
You can upload your referral securely on our website, or ask your GP to fax it to 03 8080 6484 or email it to admin@allpsychiatry.com.au
Once our friendly admin team receives your referral, it will be promptly reviewed to match you with the specialist best suited to your needs. Someone from our admin team will contact you to arrange your appointment
Neuropsychiatry bridges the gap between neurology (which focuses on the brain’s physical disorders) and psychiatry (which deals with mental health conditions). It examines how brain disorders impact mental health and behavior.
You might need a neuropsychiatric evaluation if you experience:
- Memory problems or confusion
- Personality changes
- Unexplained mood swings
- Hallucinations or delusions
- Difficulty concentrating or processing information
- Seizures with mood disturbances
Some conditions can be managed effectively with treatment, but others may require long-term care. The goal is to improve quality of life and symptom management.


